Imagine being woken at 2 a.m. by a searing, throbbing pain in your big toe — so intense that even a bedsheet touching it feels unbearable. That is gout, and it is far more common than most people realize. According to the Centers for Disease Control and Prevention (CDC), approximately 8.3 million Americans live with gout, making it the most prevalent inflammatory arthritis in adults. Once dismissed as a "disease of kings" tied to rich food and excess wine, gout is now understood as a complex metabolic disorder influenced by genetics, kidney function, diet, and medication. This guide walks you through everything you need to know.
Medical Disclaimer
This article is intended for general health information purposes only and does not substitute for professional medical advice, diagnosis, or treatment. If you have or suspect a medical condition, please consult a qualified healthcare provider.
What Is Gout? — Understanding Uric Acid Crystals
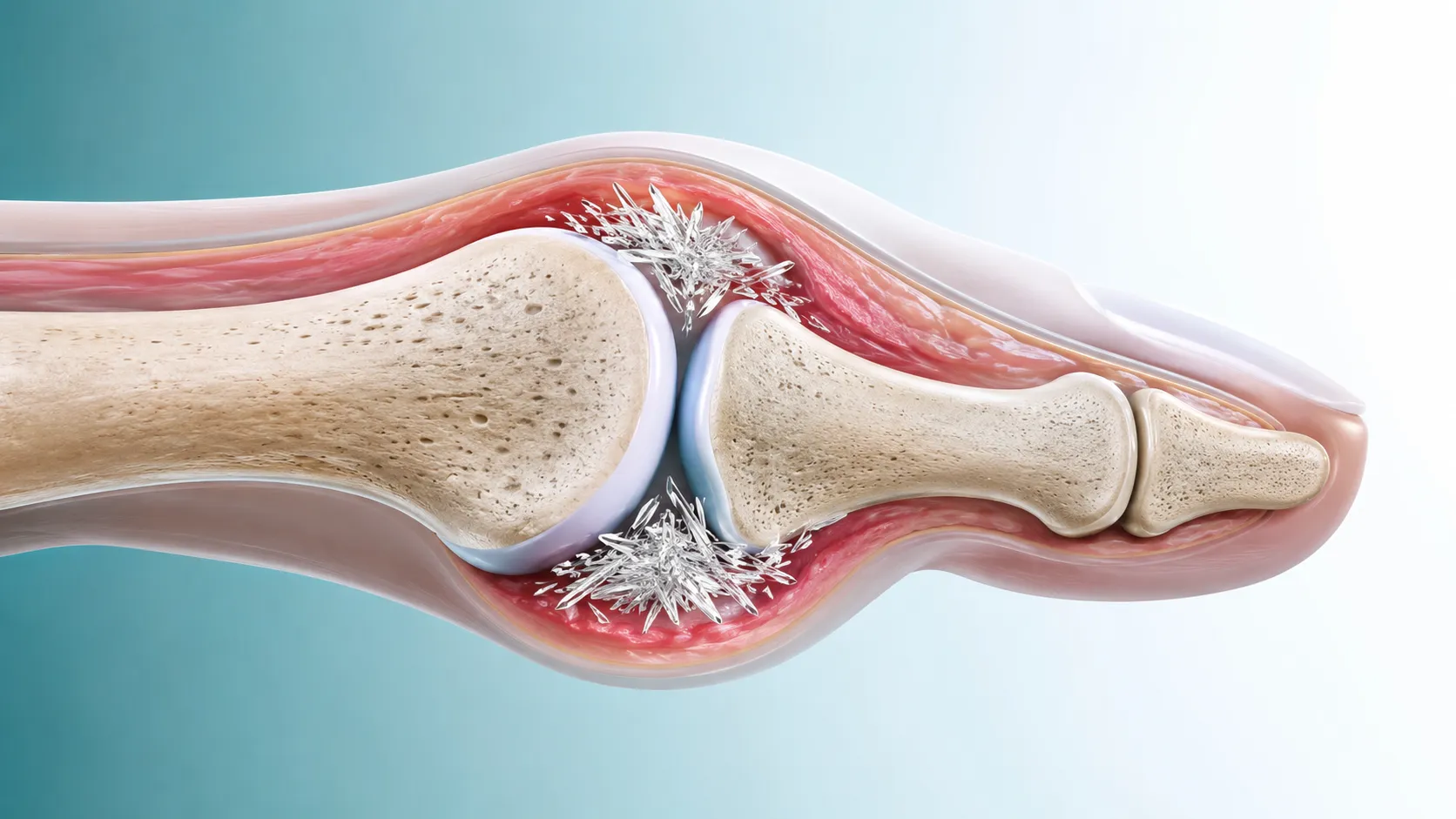
Gout is a form of inflammatory arthritis triggered by the deposition of monosodium urate crystals in and around the joints. These sharp, needle-like crystals form when blood levels of uric acid remain persistently elevated — a condition called hyperuricemia.
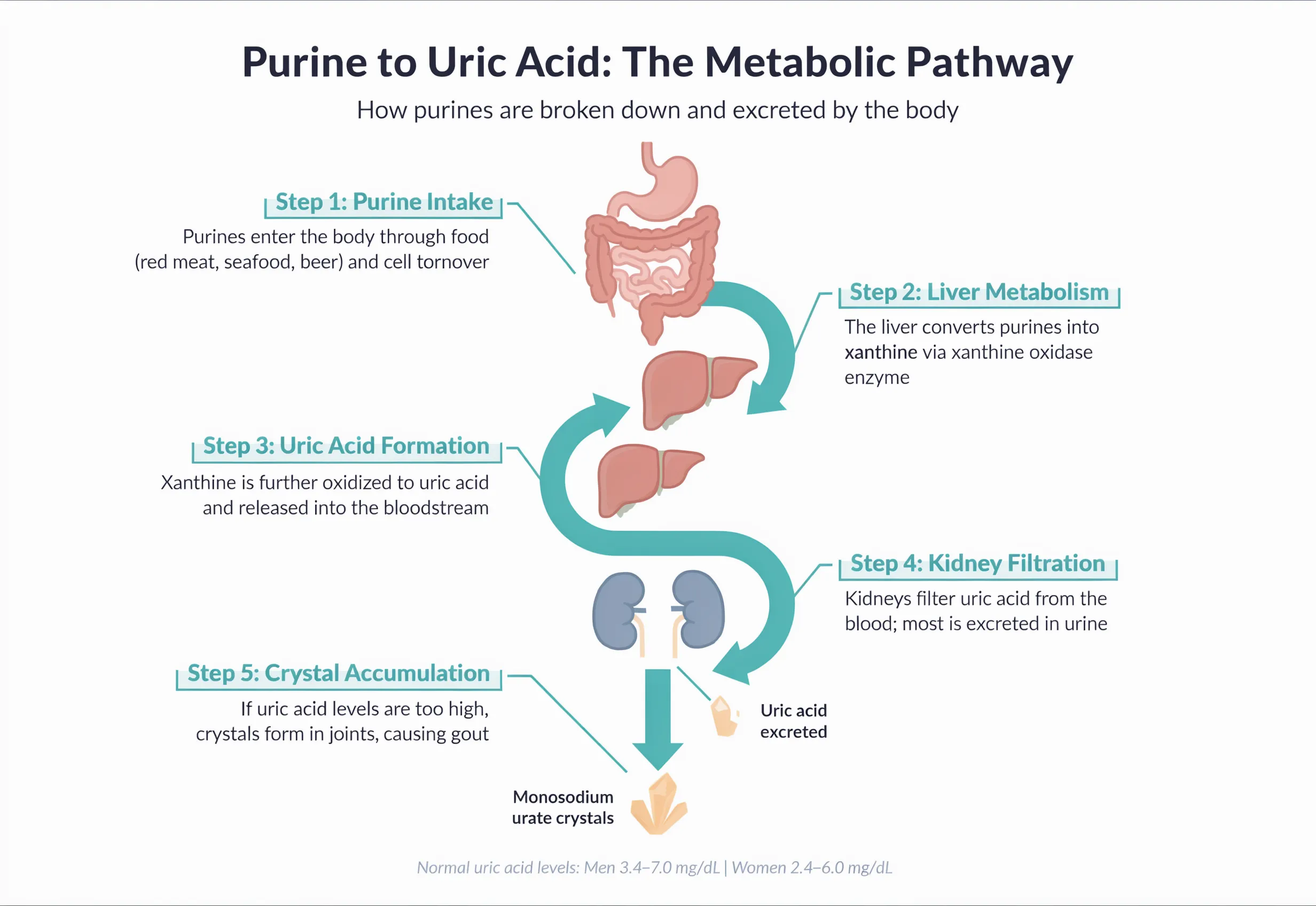
Uric acid is the end product of the body's breakdown of purines — nitrogen-containing compounds found in human cells and many foods. Under normal circumstances, uric acid dissolves in the blood, passes through the kidneys, and is excreted in urine. When either too much uric acid is produced or not enough is eliminated, it accumulates, eventually crystallizing in the cooler peripheral joints.
Blood Uric Acid Levels — At a Glance
Normal threshold: < 6.8 mg/dL (men) / < 6.0 mg/dL (women)
Normal (≤ 6.0 mg/dL)Note: A high uric acid reading alone does not confirm gout; clinical evaluation is required.
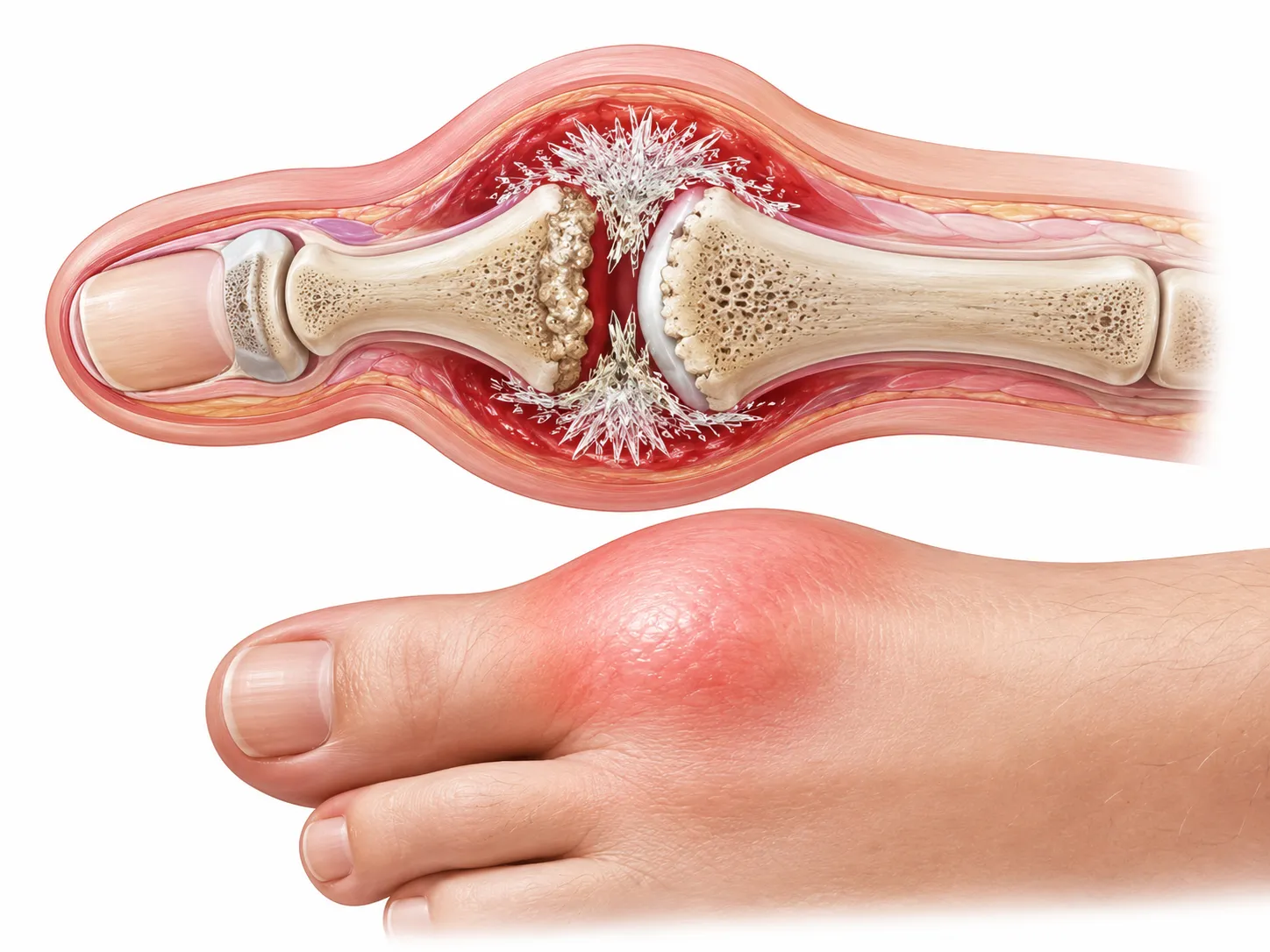
The most classic site of an initial gout attack is the first metatarsophalangeal joint (the base of the big toe), involved in up to 60% of first presentations. Other commonly affected joints include the ankle, knee, wrist, and fingers. Attacks typically strike at night, escalating to peak intensity within hours, and can last anywhere from three days to two weeks if untreated.
Causes & Risk Factors
Gout does not have a single cause. It arises when the balance between uric acid production and excretion breaks down. Several factors can tip that balance — many of which are modifiable.
High-Purine Diet
Red meat, organ meats (liver, kidneys), and certain seafood (anchovies, sardines, mussels, shrimp) are rich in purines. Fructose-sweetened beverages are a less obvious but equally important contributor.
Alcohol — Especially Beer
Beer contains purines and also inhibits renal uric acid excretion. All alcohol raises uric acid levels to varying degrees, with beer and spirits posing higher risk than moderate wine consumption.
Chronic Kidney Disease
Kidneys handle the bulk of uric acid elimination. Even mild reductions in kidney function can meaningfully impair excretion, creating a vicious cycle — gout can itself accelerate kidney damage.
Genetics
Variants in genes such as ABCG2 and SLC22A12 reduce the kidney's ability to clear uric acid. A family history of gout is one of the strongest independent risk factors.
Obesity & Metabolic Syndrome
Excess body fat raises uric acid production and lowers excretion. Insulin resistance — a hallmark of metabolic syndrome — further promotes uric acid reabsorption in the kidney tubules.
Certain Medications
Thiazide and loop diuretics, low-dose aspirin, cyclosporine, and some anti-tuberculosis drugs can each elevate uric acid by reducing renal clearance. Never stop a prescribed medication without medical guidance.
"Gout is no longer the exclusive domain of kings and aristocrats. Modern diets high in processed foods, sugar, and alcohol have democratized this painful condition." — American College of Rheumatology Clinical Practice Guidelines, 2024
Symptoms and How Gout Is Diagnosed
The Four Stages of Gout
Stage 1: Asymptomatic Hyperuricemia
Uric acid is elevated but no flares have occurred. This phase can last years — it is also the ideal window to intervene with lifestyle changes before crystal deposition begins.
Stage 2: Acute Gout Flare
Sudden-onset severe joint pain, redness, swelling, and warmth — often peaking within 12–24 hours. Even without treatment most flares resolve within 1–2 weeks, but recurrence is nearly certain without management.
Stage 3: Intercritical Gout
Symptom-free intervals between attacks. The frequency and severity of future flares generally increases over time if uric acid is not controlled, and more joints become involved.
Stage 4: Chronic Tophaceous Gout
Urate crystals accumulate as visible, firm nodules (tophi) under the skin — commonly at the ear helix, elbows, and Achilles tendon. Joint destruction and kidney stones become significant concerns.
Watch Out for Look-Alike Conditions
The acute presentation of gout can mimic septic arthritis, pseudogout (calcium pyrophosphate deposition), and rheumatoid arthritis. Accurate differential diagnosis by a physician is essential before starting any treatment.
Diagnostic Methods
| Test | What It Shows | Notes |
|---|---|---|
| Serum Uric Acid | Measures blood uric acid concentration. > 6.8 mg/dL (men) or > 6.0 mg/dL (women) is considered hyperuricemia | Simple and widely available, but may be falsely normal during an acute flare |
| Synovial Fluid Analysis | Polarized-light microscopy of joint fluid aspirate confirms needle-shaped, negatively birefringent urate crystals | The gold standard for definitive gout diagnosis |
| Dual-Energy CT (DECT) | Non-invasively maps urate crystal deposits in color-coded 3D images | Highly accurate for tophaceous gout; more expensive than other options |
| Ultrasound | Identifies the "double-contour sign" (urate coating on cartilage) and tophi | Radiation-free, bedside-ready, good for early-stage detection |
| X-ray | Reveals joint space narrowing, bone erosions, and tophi in chronic gout | Limited value in early-stage gout; normal findings do not rule out the condition |
Diet & Lifestyle Management
Diet alone typically lowers uric acid by only 1–2 mg/dL — meaningful, but often insufficient on its own. The real value of dietary changes lies in reducing flare triggers and supporting medication effectiveness. Think of food and lifestyle as the foundation that medication builds upon.
Foods by Purine Content
| Category | Representative Foods | Guidance |
|---|---|---|
| High Purine (>150 mg / 100 g) |
Organ meats (liver, kidneys, heart); dried anchovies, sardines, herring; shrimp, crab, mussels, oysters; meat-based broths and gravies; beer, spirits | Avoid as much as possible |
| Moderate Purine (50–150 mg / 100 g) |
Beef, pork, chicken (lean cuts); salmon, tuna, mackerel; legumes (lentils, chickpeas); spinach, asparagus, mushrooms | Limit to modest portions (≤ 3 oz per serving) |
| Low Purine (<50 mg / 100 g) |
White rice, bread, pasta; eggs; low-fat dairy (milk, yogurt, cheese); tofu; most vegetables and fruits; coffee and tea | Generally safe to consume freely |
What to Avoid vs. What Helps

❌ Foods to Limit or Avoid
- All alcoholic beverages (especially beer)
- Organ meats (liver, kidneys, tripe)
- Dried fish and shellfish (anchovies, shrimp)
- Fructose-sweetened sodas and juices
- Rich meat-based soups and gravies
- Processed meats (bacon, sausage)
- Large portions of red meat (> 85 g)
✅ Foods That Support Gout Management
- Cherries and tart cherry juice
- Low-fat milk, yogurt, and cheese
- Plenty of water (8+ cups / day)
- Eggs and tofu (low-purine proteins)
- Coffee (moderate intake)
- Most non-starchy vegetables
- Whole grains (oats, brown rice)
Lifestyle Habits That Make a Difference
- Stay well hydrated: Aim for at least 2 liters (roughly 8 cups) of water daily. Adequate hydration helps the kidneys flush uric acid more efficiently. A glass of water first thing in the morning and before bed is a practical starting habit.
- Lose weight gradually: Even modest weight loss can measurably lower uric acid. However, crash dieting or prolonged fasting temporarily spikes uric acid and can paradoxically trigger a flare. Aim for steady, gradual reduction.
- Choose joint-friendly exercise: Swimming, cycling, and walking are ideal — they improve metabolic health without placing excessive stress on affected joints. Rest completely during a flare; resume activity once inflammation resolves.
- Cold compress during an acute flare: Applying a cloth-wrapped ice pack to the affected joint for 15–20 minutes several times per day can blunt pain and swelling. Never apply ice directly to the skin.
- Take urate-lowering medication consistently: Do not stop prescribed medications when symptoms disappear. Discontinuation causes uric acid levels to rebound rapidly, often triggering severe rebound flares.
- Review all medications with your doctor: If you use diuretics or low-dose aspirin, inform your rheumatologist. Alternative agents may be available that achieve the same therapeutic goal with less impact on uric acid levels.
Treatment Options: Medication and Beyond
Gout treatment has two distinct, complementary goals: rapidly extinguishing the acute inflammatory flare, and chronically lowering serum uric acid to prevent future attacks and crystal deposition. These goals require different agents and should not be conflated.
Managing an Acute Gout Flare
NSAIDs
Indomethacin, naproxen, and ibuprofen are among the most effective options for rapid pain relief. Use the lowest effective dose for the shortest duration. Contraindicated in severe kidney disease or active peptic ulcers.
Colchicine
Highly effective when started within 36 hours of flare onset. Low-dose regimens (0.5 mg twice daily) are as effective as high doses with fewer gastrointestinal side effects. Safe in mild-to-moderate kidney impairment.
Corticosteroids
Oral prednisone or intra-articular triamcinolone for patients unable to tolerate NSAIDs or colchicine. Provides rapid relief but should be limited to short courses to minimize metabolic side effects.
Long-Term Urate-Lowering Therapy (ULT)
Allopurinol
The most widely prescribed ULT globally. Blocks xanthine oxidase — the enzyme that converts purines into uric acid. Patients of Han Chinese, Thai, or Korean descent should undergo HLA-B*5801 genetic testing prior to initiation due to severe hypersensitivity risk.
Febuxostat
More potent urate reduction than standard-dose allopurinol. Used when allopurinol is contraindicated or not tolerated. Requires caution in patients with established cardiovascular disease.
Probenecid
Enhances renal excretion of uric acid. Most appropriate for undersecretors with normal kidney function. Adequate fluid intake is essential to reduce kidney stone risk. Less favored in practice due to drug interactions.
Treatment Target: Serum Uric Acid < 6.0 mg/dL
Both the American College of Rheumatology (ACR) and the European Alliance of Associations for Rheumatology (EULAR) set the target serum uric acid level at below 6.0 mg/dL for most patients. For those with severe tophaceous gout, a more stringent target of 5.0 mg/dL may be appropriate. Once the target is reached, medication should generally be continued indefinitely — uric acid levels will rise again if treatment is stopped.
Key Takeaways
A gout flare is not simply a painful inconvenience — it is a warning sign that uric acid has been building silently for some time. Left unmanaged, gout can cause progressive joint destruction, kidney stones, and an elevated risk of cardiovascular disease. The encouraging counterpoint is that with consistent treatment and informed lifestyle choices, the vast majority of gout patients achieve full symptom control and protect their joints long-term.
Essential Points to Remember
- Gout results from urate crystal deposits driven by chronic hyperuricemia
- Uric acid > 6.8 mg/dL (men) signals elevated risk; confirm with synovial fluid analysis
- Organ meats, shellfish, beer, and fructose drinks are key dietary triggers
- Cherries, low-fat dairy, coffee, and adequate water intake are beneficial
- NSAIDs or colchicine manage acute flares; allopurinol/febuxostat prevent recurrence
- Target serum uric acid: below 6.0 mg/dL (5.0 mg/dL for severe cases)
- HLA-B*5801 genetic screening is recommended before allopurinol in high-risk populations
- Never stop ULT abruptly — rebound flares can be severe
One of the most common mistakes gout patients make is treating only the acute attack while neglecting the underlying hyperuricemia. The pain may disappear on its own, but the crystals do not. Treat each flare as a prompt to revisit your urate-lowering strategy with your doctor. Managing gout is not a sprint — it is a lifelong commitment to keeping your uric acid at a healthy level. With the right tools and guidance, that goal is entirely achievable.
Medical Disclaimer
This article is intended for general health information purposes only and does not substitute for professional medical advice, diagnosis, or treatment. If you have or suspect a medical condition, please consult a qualified healthcare provider.