Have you ever woken up in the morning to find your finger stuck in a bent position, making a distinct clicking sound as you try to straighten it? What starts as minor morning stiffness can escalate to a finger that locks completely — the hallmark of Trigger Finger Syndrome, medically known as Stenosing Tenosynovitis. More common than many people realize, trigger finger affects roughly 2–3% of the general population over a lifetime, and it's highly treatable when caught early.
This article is intended for general health information purposes only and is not a substitute for professional medical diagnosis, advice, or treatment. If you are experiencing symptoms of any medical condition, please consult a qualified healthcare provider.
What Is Trigger Finger Syndrome?
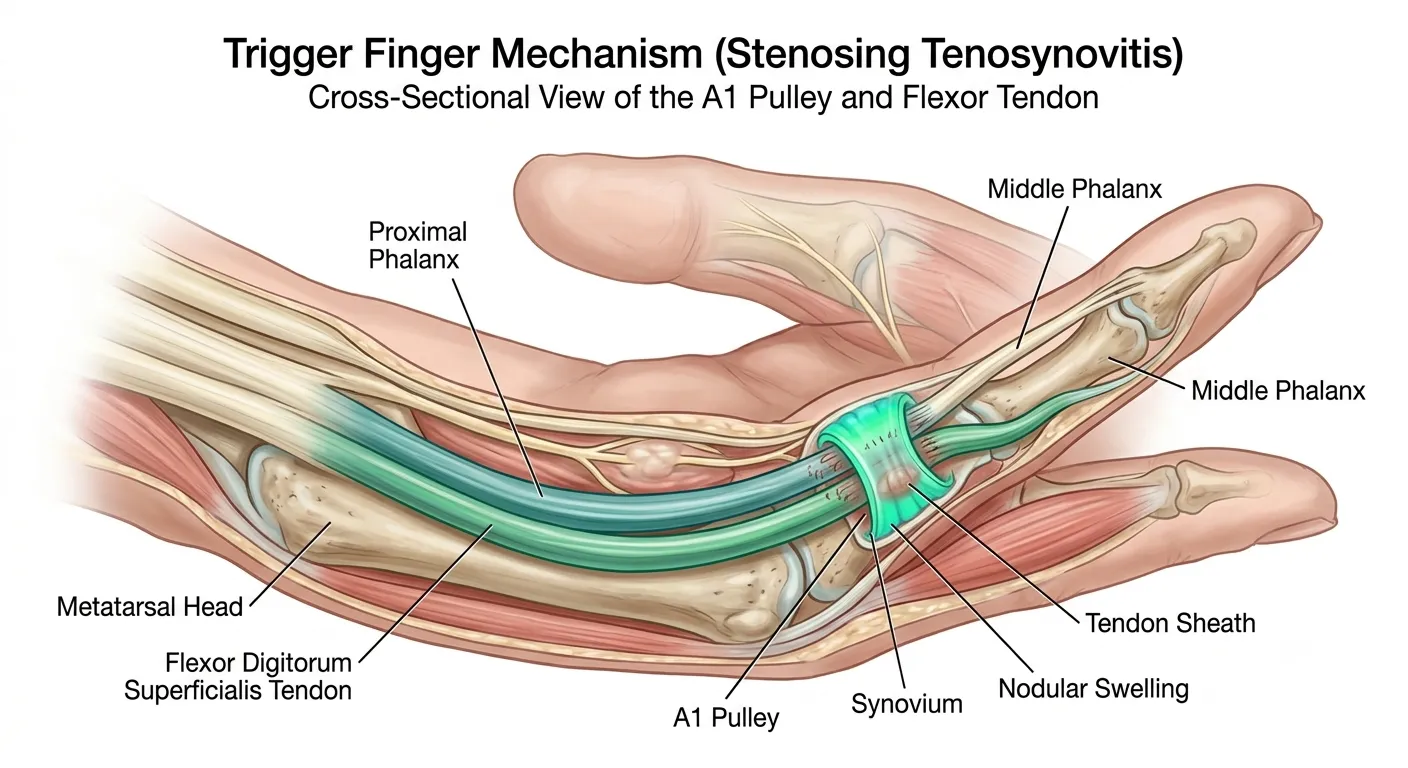
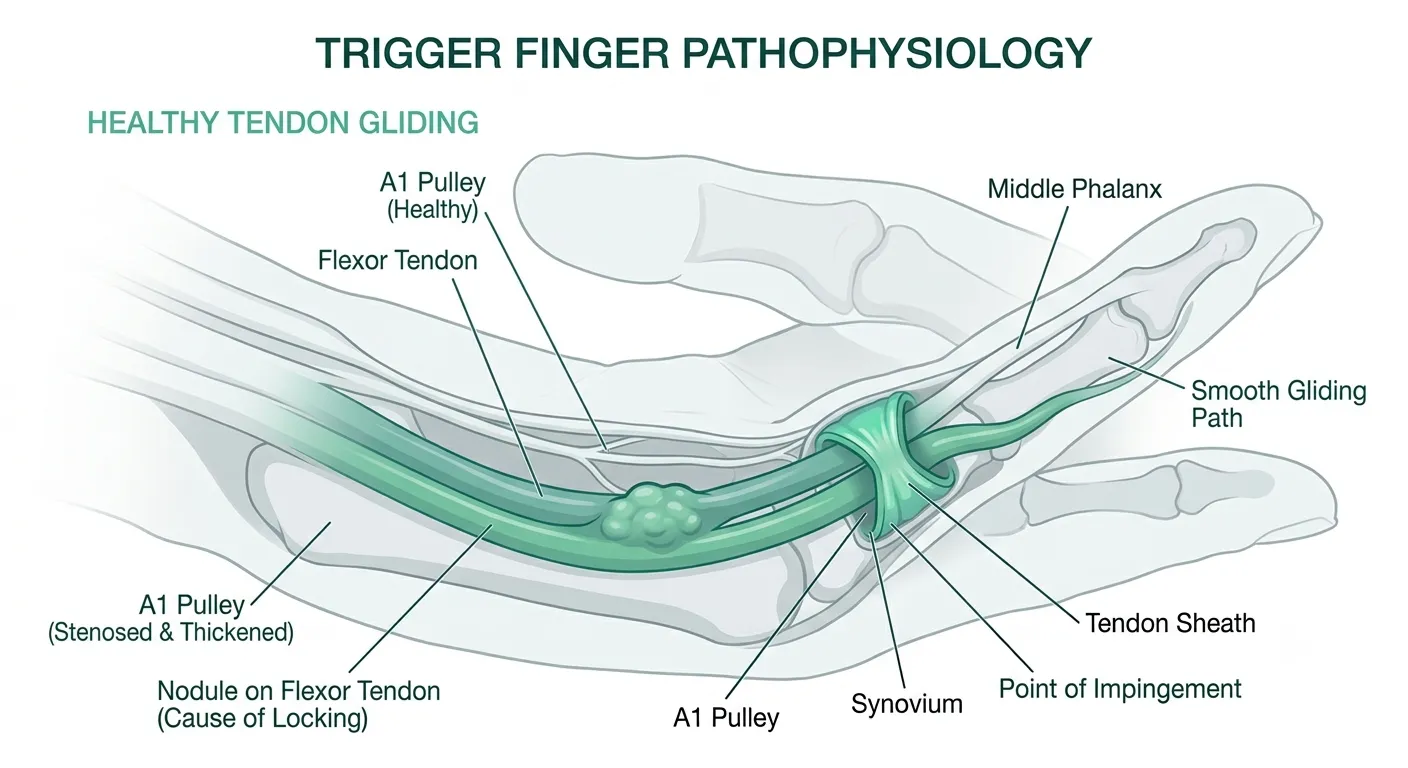
Trigger finger occurs when the flexor tendon — the structure that bends your finger — gets caught in a narrowed or thickened fibrous ring called the A1 pulley. This pulley acts as a sheath entrance at the base of the finger. When the pulley thickens or a nodule develops on the tendon, the tendon can no longer glide smoothly. The result: that familiar click, snap, or lock that gives the condition its evocative name.
According to data published in hand surgery specialty journals, approximately 2–3% of the general population will experience trigger finger at some point in their lives. The prevalence is notably higher among women aged 40–60 and individuals with diabetes.
Key Insight
When detected early (Stage 1–2), trigger finger often responds well to non-surgical treatments. Waiting until the finger locks completely (Stage 3–4) significantly reduces the effectiveness of conservative options.
Causes & Mechanism
Flexor tendons travel through a fibrous tunnel called the tendon sheath from the palm all the way to the fingertip. At the palm-side base of each finger sits the A1 pulley, the tunnel's entrance ring. Chronic friction or inflammation causes the pulley to thicken, and a nodule can form on the tendon itself. When that nodule is too large to pass through the narrowed pulley opening, the finger catches or locks — the defining mechanical failure of trigger finger.
Key Contributing Factors
What Raises Your Risk
- Repetitive hand use: Prolonged gripping — power tools, musical instruments, scissors, prolonged smartphone scrolling — creates ongoing friction at the A1 pulley
- Diabetes mellitus (Type 1 & 2): Poor glycemic control promotes fibrosis in tendon tissue. Diabetic patients face a 10–20% higher incidence compared to the general population
- Rheumatoid arthritis: Systemic inflammation of joints and tendon sheaths can trigger secondary pulley thickening
- Hypothyroidism: Thyroid deficiency promotes mucin deposition in connective tissue, contributing to pulley stenosis
- Gout & renal disease: Urate crystal deposition near tendons causes localized inflammation
- Pregnancy & breastfeeding: Hormonal fluctuations cause ligament and tendon laxity that can affect pulley function
- Genetic predisposition: Anatomically narrower pulleys or inherently thicker tendons can run in families
The American Academy of Orthopaedic Surgeons (AAOS) notes that certain occupational groups — farmers, musicians, occupational therapists, seamstresses — show meaningfully higher rates of trigger finger than the general public, reflecting the outsized role of repetitive gripping in the pathology.
Symptoms & 4-Stage Classification
Trigger finger typically progresses gradually. Most patients experience mild morning stiffness at first, only to find months later that the finger stubbornly refuses to open without help. Hand surgeons use the Quinnell (Green's modification) grading system to classify severity into four stages.
Intermittent aching or stiffness at the base of the finger, especially in the morning or after rest. No catching. Resolves naturally with movement.
The finger catches or clicks during flexion or extension, but the patient can actively unlock it. Tenderness on pressing the A1 pulley area in the palm.
The finger locks in a bent position and must be passively straightened with the other hand. Significant pain accompanies the forced extension.
The finger is permanently fixed in flexion. No passive or active extension is possible. Surgical intervention is required without delay.
Symptom Checklist
- Pain or stiffness at the base of the finger (palm-side) after waking up
- A distinct clicking, popping, or snapping sensation when bending or extending a finger
- Tenderness when pressing the palm at the base of the affected finger
- Stiffness that eases after the finger "warms up" with activity
- A finger bent at the middle joint that cannot be straightened without assistance (Stage 3+)
- Ring finger, thumb, or middle finger most commonly affected
"Trigger finger almost always begins with nonspecific morning stiffness that patients dismiss as 'sleeping on it.' That early window — before locking begins — is when intervention requires the least." — Adapted from the Korean Society for Surgery of the Hand clinical guidelines
Risk Groups & Statistics
Trigger finger can strike anyone, but certain groups carry a substantially elevated risk:
| Risk Factor | Relative Risk | Mechanism |
|---|---|---|
| Women aged 40–60 | 6× vs. men | Hormonal shifts & anatomical differences |
| Diabetes (Type 1 & 2) | 10–20% higher | Accelerated tendon fibrosis |
| Rheumatoid Arthritis | Significantly elevated | Systemic inflammation of tendon sheath |
| Hypothyroidism | 2–3× higher | Mucin deposition thickening tissue |
| Repetitive gripping occupations | 3–5× higher | Chronic friction on A1 pulley |
| Prior De Quervain's tenosynovitis | Co-occurrence likely | General tendon disease susceptibility |
Trigger finger in children: Pediatric trigger thumb is a distinct entity, usually a congenital anomaly of the tendon sheath discovered between ages 1–3. Unlike adults, spontaneous resolution is possible — watchful waiting is often the first approach before surgical release is considered.
Diagnosis
The good news: trigger finger is primarily a clinical diagnosis, meaning a skilled hand specialist can diagnose it from history and physical exam alone. Additional imaging becomes relevant when co-existing conditions or atypical presentations are suspected.
Diagnostic Process Step by Step
-
1History-Taking Duration of symptoms, aggravating activities, occupational hand use, presence of diabetes or thyroid disease, prior hand injuries.
-
2Physical Examination Direct palpation of the A1 pulley for local tenderness; assessment of active and passive range of motion; checking for catching or locking in real-time.
-
3Ultrasound (when indicated) Measures A1 pulley thickness, visualizes tendon nodule size, and assesses inflammation — all without radiation exposure. Increasingly preferred for guided injections.
-
4X-Ray Not diagnostic for trigger finger itself, but useful for ruling out arthritis, gout tophi, or fractures that might mimic or accompany the condition.
-
5Blood Tests Ordered when underlying systemic disease is suspected — rheumatoid factor, HbA1c (blood sugar control), thyroid-stimulating hormone (TSH).
Complete Treatment Comparison
Treatment decisions hinge on the severity stage and the patient's overall health. The general principle is to start conservatively and escalate only when needed.
Conservative Management
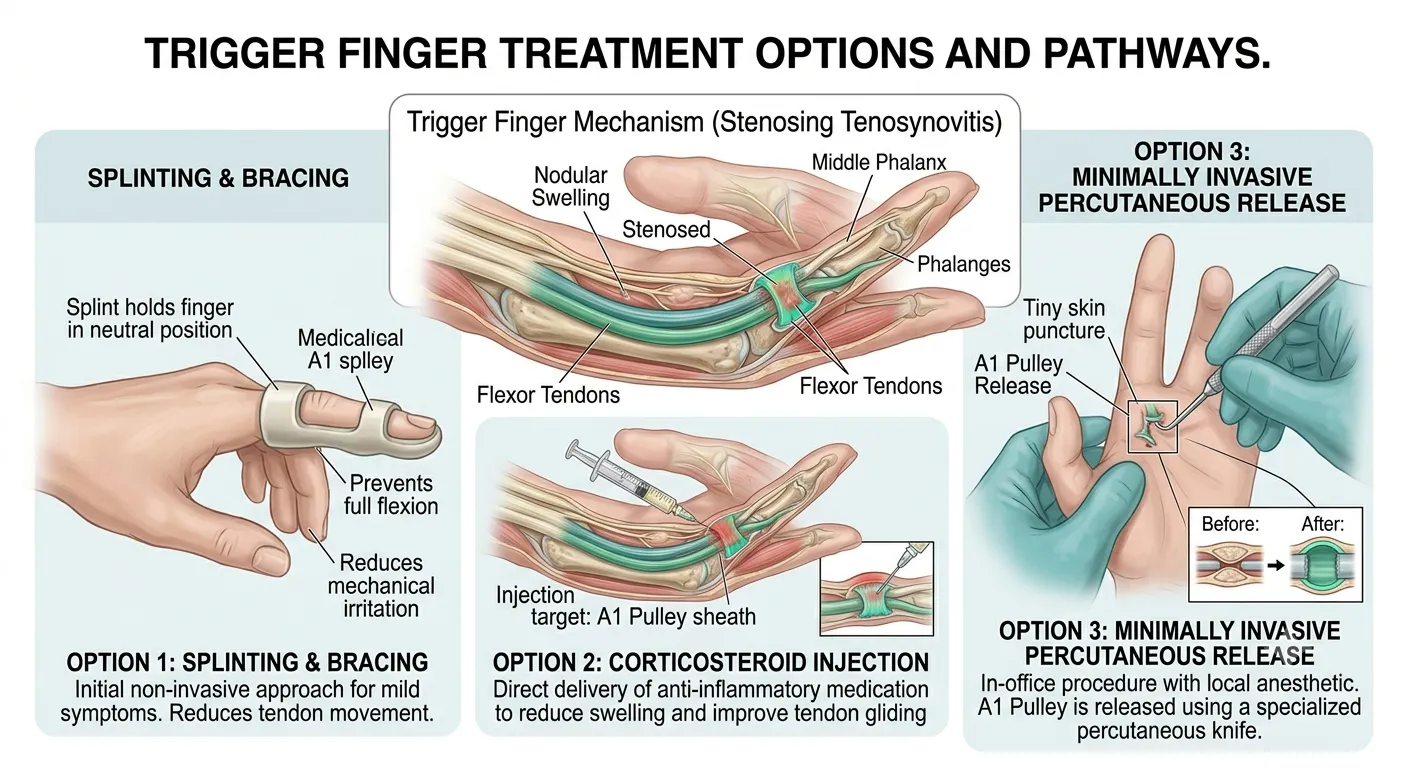
Activity modification, splinting (usually a resting night splint), oral NSAIDs, heat/ice therapy, and stretching exercises. Best suited for Stage 1 and mild Stage 2 presentations.
First-LineCorticosteroid Injection
Triamcinolone or methylprednisolone is injected directly around the A1 pulley to rapidly reduce inflammation. A single injection achieves symptom resolution in 50–70% of cases; a second injection can be given if the first provides partial relief.
Second-LinePercutaneous Release
A needle tip is used under ultrasound guidance to divide the A1 pulley without an incision. Faster recovery than open surgery, with a success rate of approximately 80–90%. Increasingly preferred for Stage 2–3 patients who don't respond to injections.
Mid-LevelOpen Surgical Release
A small incision is made in the palm under local anesthesia to directly cut the A1 pulley. The gold standard: greater than 95% cure rate. Preferred for Stage 3–4 or when other treatments have failed.
DefinitiveSide-by-Side Treatment Comparison
| Treatment | Success Rate | Procedure Time | Recovery | Main Downside | Best For |
|---|---|---|---|---|---|
| Splint + Rest | ~50–60% | Ongoing (4–6 wks) | Immediate daily life | High recurrence, long commitment | Stage 1 |
| Steroid Injection (×1) | ~50–70% | 5–10 min | Days to weeks | Tendon weakening with repeats; blood sugar spike in diabetics | Stage 2–3 |
| Percutaneous Release | ~80–90% | 10–15 min | Days to 1 week | Small nerve injury risk; requires ultrasound guidance | Stage 2–3 |
| Open Surgical Release | >95% | 15–30 min | 2–4 weeks | Incision scar; higher upfront cost | Stage 3–4 |
A note for diabetic patients: Corticosteroid injections can temporarily elevate blood glucose for 24–72 hours. Patients with poorly controlled diabetes should discuss this with their endocrinologist before proceeding. Some literature suggests that diabetic patients may achieve lower success rates from injections, making earlier consideration of surgical release reasonable in this group.
Post-Surgery Recovery & Rehabilitation
Most patients return to routine daily activities within 2–4 weeks after open surgical release. Occupational therapy-guided rehabilitation significantly shortens this timeline and reduces the risk of stiffness.
Recovery Timeline After Open Release
| Timeframe | Status | Recommended Actions |
|---|---|---|
| Surgery day | Dressing applied, hand elevated | Begin gentle finger movements |
| Days 1–3 | Swelling & pain control phase | Ice packs, oral pain medication |
| Week 1–2 | Suture removal (if applicable) | Light ADLs, begin occupational therapy |
| Week 2–4 | Near-full active motion restored | Return to normal life, gradual load increase |
| Week 4–8 | Full recovery | Return to work, sport restrictions lifted |
Some patients experience temporary post-operative stiffness — a normal part of healing that responds well to guided exercises. Scar hypertrophy causing secondary restriction is rare, but when it occurs, scar massage and thermoplastic splinting by an occupational therapist are highly effective.
Home Care & Self-Management
For mild Stage 1–2 symptoms, diligent home care can produce meaningful improvement. These measures complement — but never replace — professional evaluation.
Core Home Management Principles
- Reduce or temporarily avoid activities that trigger pain or stiffness
- Apply ice packs (up to 20 minutes) for acute swelling; use a warm soak for chronic stiffness before stretching
- Use a finger extension splint overnight to hold the finger in a straight position
- OTC NSAIDs (ibuprofen, naproxen) can reduce pain and swelling short-term — consult a doctor for use beyond 7–10 days
- If no improvement after 2–3 weeks of self-care, schedule an appointment with a hand specialist
Night Splinting: How It Helps
A nighttime extension splint holds the finger in a neutral (straight) position during sleep, reducing stress on the flexor tendon and A1 pulley during the body's natural repair window. Research has found that 6 weeks of consistent night splinting resolves symptoms in approximately 55–70% of patients with mild-to-moderate trigger finger. Importantly, wearing the splint only at night preserves daytime hand function and prevents muscle weakening.
Heat vs. Ice: When to Use Which
- Ice (Cryotherapy): For acute flare-ups, swelling, and sharp pain. Apply for 15–20 minutes, 3–4 times daily. Always wrap in a cloth — never apply ice directly to skin.
- Heat (Warm Soak): For chronic stiffness and before stretching. Soak in warm water (38–40°C / 100–104°F) for 10–15 minutes to increase tissue flexibility.
- Contrast Therapy: Alternating heat (3 min) and ice (1 min) for 15 minutes can improve local circulation when stiffness is the primary complaint.
Prevention Stretching Routine
The following exercises help maintain flexor tendon flexibility and improve circulation around the A1 pulley. If your finger is currently locked (Stage 3–4), please perform these only under professional guidance to avoid injury.
6-Step Prevention & Rehab Stretch Routine
-
1Finger Extension Stretch Place your hand palm-down on a flat surface. Gently press fingers flat against the surface and hold for 5 seconds. Release and repeat 10 times × 3 sets. Prevents flexor tendon shortening.
-
2Passive Finger Extension Use your opposite hand to gently straighten the affected finger. Hold 15–20 seconds, 3–5 times daily. Reduces adhesion formation in the tendon sheath.
-
3Finger Abduction (Spread) Fully extend your hand and spread fingers apart as wide as possible, then bring them together. 15 reps × 3 sets. Strengthens intrinsic hand muscles.
-
4Tendon Gliding — O-Ring Touch each fingertip to the thumb tip one at a time to form an "O," then fully extend. 5 reps per finger. Directly improves flexor tendon gliding through the pulley.
-
5Wrist Rotation Slowly rotate your wrist clockwise 10 times, then counterclockwise 10 times. Improves overall hand circulation and reduces forearm tension that can transmit to the fingers.
-
6Slow Fist — Make & Open Gently and slowly form a fist, hold 3 seconds, then fully extend all fingers. 10–15 reps × 2 sets. Perform only within a pain-free range of motion.
Smartphone habit tip: Single-handed phone gripping places sustained pressure on the ring and little fingers. A popsocket, ring holder, or phone stand distributes force away from the A1 pulley. Add a 30-second finger stretch every 30 minutes of screen time — a small habit with outsized protective benefits.
When to See a Doctor Immediately
Seek Prompt Medical Attention If:
- Your finger is locked in a bent position and you cannot straighten it at all
- Even forceful passive extension by your other hand fails to open the finger
- You experience sudden severe pain accompanied by swelling and warmth
- Two to three weeks of self-care produce zero improvement
- Multiple fingers develop locking simultaneously (possible systemic disease)
- You notice redness, fever, or discharge from the finger area (possible infection)
While trigger finger is not life-threatening, progression to Stage 3–4 makes treatment significantly more complex and recovery lengthier. For professionals who rely on manual dexterity — surgeons, musicians, mechanics, athletes — early specialist consultation is not overcaution, it's strategic.
Which Specialist Should You See?
- Orthopedic Hand Surgeon: The most appropriate first choice for comprehensive evaluation, including the full spectrum of treatment from injection to surgery.
- Physical/Occupational Therapist: Ideal for conservative rehabilitation, splint fabrication, and exercise-based management of Stage 1–2 cases.
- Rheumatologist: When rheumatoid arthritis or another systemic inflammatory disorder is the suspected underlying cause.
- Endocrinologist: When diabetes or hypothyroidism is suspected as a contributing factor requiring better systemic control.
Key Takeaways
Trigger finger is more common than most people realize — and more treatable than many fear. Here's the bottom line:
Everything You Need to Remember
- Trigger finger is caused by A1 pulley narrowing that prevents smooth flexor tendon movement
- It progresses through 4 stages: stiffness → catching → locking → fixed deformity
- Women 40–60, diabetics, and repetitive grip workers are at highest risk
- Stage 1–2 can often be managed with splinting, rest, and targeted stretching
- A single corticosteroid injection resolves symptoms in 50–70% of patients
- Open surgical release carries over a 95% cure rate and is safe under local anesthesia
- Don't wait until the finger locks — early treatment means simpler, faster recovery
Your hands are involved in nearly everything you do. If you're experiencing even mild symptoms, today is the right day to start the prevention stretching routine above and reduce repetitive gripping where possible. A few minutes of daily hand care can protect decades of function.
This article is intended for general health information purposes only and is not a substitute for professional medical diagnosis, advice, or treatment. If you are experiencing symptoms of any medical condition, please consult a qualified healthcare provider.